Ring the changes
Fifty years ago the Pill was made freely available to women, giving them reproductive freedom and control. But is it information rather than hormones that will power the next era of family planning?
Although the contraceptive Pill became available in the UK in 1961 and by 1964 half a million women were taking it, they were still the lucky few. You needed a GP who deemed you worthy of it and needed to be a married women for whom pregnancy posed a health risk. And you needed two shillings a week to pay the subsidised cost.
It was the 1967 NHS Family Planning Act – 50 years old this week – that replaced the patchwork of services all over the country and made contraception readily available to the masses. But although the act brought women hard-won reproductive freedom, that’s not always how the argument was framed, nor was it clear at the time that hormone-based contraceptives could have such powerful side-effects.
“Prior to the act contraceptive services were patchwork. There was no uniformity so that was the big thing – that the country was treated as a whole,” says political historian Clare Debenham. “The act really did give women legitimacy to seek help. It wasn’t a back-street venture – you had a right to family planning. It took it from the shadows and into
the open.”
“Low income groups that were reproducing. They didn’t say this is the women’s right – it was an economic argument.”
Calls for better access to birth control go back to women who entered the campaign rather than “returning to their knitting and coffee mornings” after winning the right to vote, according to Debenham, who adds that their methods for limiting their family prior to the act were “fairly horrific”.
She says: “Many women were at their wits’ end and they used to jump from the slop stone in the kitchen or off the seventh step to try and end their pregnancy because they were desperate. It was frightening and it wasn’t particularly effective.
“They didn’t trust their husbands with condoms and they didn’t seem to like them using them. The advent of the Pill gave the ability to women to control a pregnancy rather than relying on a husband.”
The act was one of a flurry of liberalising reform measures at the time, with home secretary Roy Jenkins and health secretary Kenneth Robinson lending their support to the legalisation of abortion, the decriminalisation of homosexuality and the easing of censorship laws. But although the benefits of the Family Planning Act were vast, Debenham says the male-dominated Labour government wasn’t acting in the interests of female liberation.
“It really was a eugenic argument that Edwin Brooks used when he introduced it as a Private Member’s Bill. He identified it as a social problem – low income groups that were reproducing. They didn’t say this is the women’s right. He put forward an economic argument.”
The introduction of injectable contraception in 1974 was followed by the implant, hormone-releasing coils, vaginal rings and patches, all of which have increased women’s contraceptive choice. Today around 3.5 million women use some form of hormone-based contraception in the UK. The Pill remains the most popular – with 45 per cent of all contraception users opting for it. For many, it’s a calculated risk.
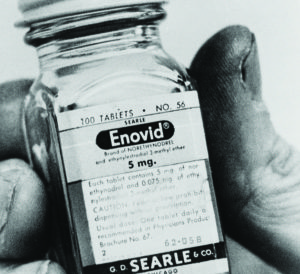
Around 12 women per 10,000 taking combined oestrogen and progesterone contraception are thought to be at risk of deep vein thrombosis or pulmonary embolism per year. The risk is low but the consequences serious and have been known from the beginning. The first large-scale human trial of the Pill was conducted with ill-informed women in Puerto Rico in the 1950s. Its success in preventing pregnancy overshadowed the three deaths that occurred during it. They were not reported as being connected or investigated, despite strong circumstantial evidence suggesting the high-dose of oestrogen was making the women susceptible to blood clotting. The Pill was legalised in America in 1957 before making its way to the UK.
“We’re now on the third generation of the Pill so it’s very different to it was when it first came out. It would be difficult to say they should have waited [for more research]. For the time it was the right thing,” says Natika Halil, CEO of the Family Planning Association, which has published reports funded by hormone contraceptive manufacturers.
“We’ve learnt more so the risk factors are very clearly identifiable. For example, if you’re a woman over the ago of 35 and you smoke you have risk indicators and you wouldn’t be prescribed the Pill.”
But concerns over side-effects remain, highlighting how the development of the Pill for women took place in very different cultural and social times from now. Most of the research about female contraception has happened in real time while the male pill, which has been in development as long as the female version, is continuing to be advanced behind the scenes. Last year a medical trial of a 96 per cent effective male injection was halted after 30 of the 230 participants reported “intolerable” side effects. They included acne, mood swings and changes in libido and it was decided more research was needed. The same symptoms are all found in women taking widely available contraception that has been on the market for decades.
Other symptoms include nausea, breast tenderness and headaches. Women who use hormonal contraceptives are more likely to be treated for depression. Patient leaflets warn to be on guard for blood clotting. They also include weight gain as a common side-effect, although reviews of research find little evidence of this.
On the other hand, after years of concerns about a link between the combined pill and breast and cervical cancer, a 44-year study revealed in March no overall risk. The risk of ovarian, endometrial and bowel cancer is reduced. The study, set up by the Royal College of General Practitioners in 1968, also found other benefits including help with premenstrual symptoms and a reduction in menopausal symptoms in some women.
“I have used the combined pill, which didn’t work as I fell pregnant with my second child whilst on it,” says Emma Livingstone, a mother of five from the Isle of Wight. “I then had the depo injection, which was awful and made me bleed constantly, making me ill and anaemic. It also made me depressed.
“I didn’t know the injection was causing the bleeding until I saw the doctor, who was reluctant to stop the injections. She actually talked me into having it twice more. I then went back onto the Pill a few years later but I started getting migraines so I was taken off it. I was offered the coil, which I rejected as I was sick of putting hormones into my body and my mum had fallen pregnant using the hormone-free one.”
“I don’t know why I took hormones for so many years. If I knew then what I know now I wouldn’t have even thought about taking it.”
Livingstone began to teach herself natural family planning methods, which involve abstaining from sex or using alternative protection on fertile days (usually around three per month). She did it by charting her basal body temperature and cervical fluid on a fertility app. She regrets the years spent using hormonal contraception and wishes she had known about natural methods years ago.
“It worked fantastically for me and it was great learning so much about my body and what’s going on at each point during my cycle. It has also helped me understand why I might be feeling anxious or tired during different parts of my cycle. I struggle with my anxiety and it really helps to know there is a hormonal contribution.”
Office of National Statistics surveys between 2001 and 2009 showed that 26 per cent of women took the Pill compared with only 2 per cent who opted for natural family planning, despite the NHS and FPA both claiming the two methods are equally effective – 99 per cent – although that’s only if the natural method is adopted perfectly.
Halil says the lack of support for natural family planning is a funding issue. “There are professionals in the field who are real advocates of it and say if it is taught properly it really works. But you do have to be taught it – I think there should be more known about it.”
Halil says it wouldn’t be as simple as redirecting NHS funds away from Pill prescriptions and into education since contraception receives very little money anyway and many local authorities have decreased what little budget they have following cuts to public health budgets.
Like Livingstone, many other women are taking education about their bodies into their own hands. Since it launched in the UK in February 20,000 users have begun natural family planning with Natural Cycles – an app certified across Europe as a medical device to be used as contraception.
Created by Swedish husband and wife team Dr Raoul Scherwitzl and Dr Elina Berglund – one of the scientists who discovered the Higgs Boson – the app’s algorithm helps women pinpoint their fertility and the safe days to have sex. Women are required to take their daily temperature and input it into the app – as little effort as remembering to take
the Pill.
Sara Flyckt has been using Natural Cycles, which was launched in Sweden first, for four years.
“I used the depo injection for nearly 10 years and I was on the Pill for a couple of years. Then I got pregnant and I got talked into using the mini pill afterwards,” she says. “I could start crying for nothing and I knew it was down to the Pill. I wanted to come off it but the coil scared me and everything else had so many hormones so when I found out about this it seemed ideal.

“It’s changed my mood swings and I’ve become more aware of my body and my cycle and when to look out for PMS.
“I don’t know why I took hormones for so many years. It was the easiest and seemingly most secure option but if I knew then what I know now I wouldn’t have even thought about taking it.”
Scherwitzl says: “What women who use the product say most commonly about the product is that they feel empowered. Just like the Pill empowered women in the 1960s to have that freedom, they’re now being empowered by gaining the knowledge. It’s extremely comforting to understand how your body is working.”
Scherwitzl says women can use Natural Cycles with no prior knowledge of their cycle.
“When you start you just need to understand how to measure temperature and understand red and green. Then over time the app educates the woman on ovulation and menstruation and they get to know this language. Our users, when they discuss their data in forums, they speak like gynaecologists.
“The NHS has put a lot of money into providing contraception for free and increasing knowledge of it and I think the second part is to offer something equally important – inform people on how it works so then they can make informed choices on something as important as having a child or not.”
In Sweden Natural Cycles has a 4 per cent contraceptive market share – comparable with the IUD in the UK. Scherwitzl claims the app and its sophisticated use of data transform what has been seen as an ineffective method to bring about a new era in contraception.
“Everyone in the research community welcomes Natural Cycles because it’s an addition, another choice for women, and they see that many women in their twenties and thirties start to abstain from hormonal contraception and that could be a worrying trend,” he says.
“Instead of chemicals or drugs we have information to empower women so I do think the information age is coming to this field.”


Leave a reply
Your email address will not be published.